

















DME Fraud: The Undead Zombie of Healthcare Fraud
- May 11, 2026
- 0
- 6 min read
Sponsored Content
Durable Medical Equipment (DME) consists of things like knee braces, back braces, glucose monitors, wheelchairs, and any other medical equipment prescribed for a patient. For providers, prescribing and distributing DME is not a one-time transaction, they are healthpayer billing streams. Unlike other healthcare services provided, such as fee-for-service, DME offers providers high reimbursement rates, repeatable billing, very low clinical scrutiny, and very low real-time claims validation. In fact, DME fraud is perfect because DME rarely requires direct physician oversight, in-person patient visits, or the complex preauthorization required by some other specialty care.
For criminals perpetrating this type of healthcare fraud, DME fraud is viewed more as recurring revenue than actual healthcare. It’s possibly the path of least resistance for fraudsters because required documentation can be easily templated, the actual medical necessity of DME equipment only needs to be loosely justified, and once a supplier is enrolled and begins billing they are assumed to be legitimate until they prove otherwise.
The Supply Chain Behind the Scheme
DME fraud is more often a coordinated system similar to legitimate workflows, less often a solo operation. DME fraud consists of the familiar supply chain steps found in other types of healthcare fraud.
Fraudsters use call centers and TV ads to target Medicare beneficiaries with free scooters or support braces to engage their unwitting participants to collect enough beneficiary information to provide the service. Some of the patients recruited knowingly participate, not fully understanding what they are agreeing to, as their identities are then used for fraudulent purposes. According to the DOJ, providers are often paid per order to approve DME prescriptions with little or no actual patient interaction. DME providers then bill Medicare for unnecessary or ghost equipment, and billing aggregators and shell companies distribute claims across multiple entities to disguise any suspicious pattern of billing.
DME fraud follows the same high-volume playbook of some of the other healthcare fraud types. That playbook isn’t theoretical. In a 2019 case involving over $1.2 billion in fraudulent claims, call centers targeted Medicare beneficiaries, telehealth providers generated prescriptions, and DME companies billed for unnecessary back and knee braces. The scheme worked because medical necessity wasn’t validated prior to payment, and the process of filing the claim was never challenged.
Telehealth as a Fraud Accelerant
Telehealth removed the friction and limits associated with DME fraud. No longer were DME providers limited to the number of patients they could physically interact with any given day. Because of telehealth, orders could be signed remotely and interactions became minimal or even fabricated entirely.
Fraudulent providers could approve hundreds of DME orders in a single day. And telehealth could be used to facilitate the distribution of unnecessary equipment equating to hundreds of millions in claims.
In 2020, DOJ’s Operation Rubber Stamp exposed $4.5 billion in telehealth-driven fraud, much of it tied to DME. Providers were paid to sign off on orders without even seeing patients, sometimes approving requests in seconds. Telehealth didn’t just enable fraud, it removed the natural limits that once contained it.
The Fraud Control Gap
The healthcare industry still operates in a pay-and-chase fraud control operating model. And DME fraud providers are able to exploit that. There is still a difference between what healthpayers are able to validate, such as patient identities and provider NPI numbers, and what they are less able to validate, such as whether providers are actually seeing patients, or whether the equipment they are prescribing is actually necessary.
Within DME transactions, healthpayers are able to confirm that a patient exists and the patient identity is correct. They can also verify that the DME provider is credentialed and that the billing code the provider is using is valid. The healthpayers, however, have a harder time verifying that whether the equipment was even needed, whether it was delivered, or if the clinical interaction with the patient was legitimate.
By the time healthpayers are able to answer these questions about DME claims, the claim has already been paid.
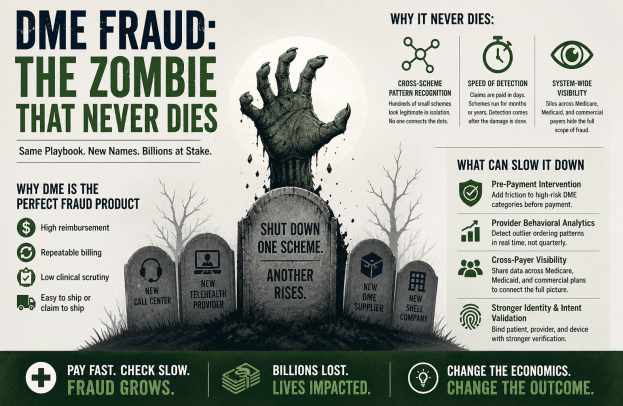
Why It Never Dies
The existence of DME fraud continues because of the economics of DME fraud. The deck is stacked in favor of the crooks as reimbursements happen quickly, detection of the fraud lags months or years, fraud recoveries are only partial, and new entities can be rapidly created as bad ones are shut down.
DME fraud in healthcare is similar to a zombie attack – you shut one scheme down, prosecute the operators, and recoup some of the money lost and you think it’s over. Then a new version appears with the same patterns, same playbook, but different names and different shell companies. DME fraud doesn’t persist because it’s hard to detect, it persists because the same model still works.
The scale of that persistence is clear. In 2025, the DOJ announced a record $14.6 billion healthcare fraud takedown, again with DME and telehealth at the center. These weren’t new tactics, but instead from the same playbook, repeated across fragmented schemes that weren’t connected quickly enough, detected early enough, or viewed across the full system.
What Can Slow Down DME Fraud
Even though the healthcare industry still fights its fraud using the pay-and-chase method, there has been some traction for advanced technologies and new best practices. For DME fraud specifically, the industry should focus on three key fraud-fighting tactics.
Healthpayers should deploy a pre-payment intervention capability that targets the higher-risk DME categories with more stringent validation before claims are paid. Adding even limited friction to the claims process could disrupt some of the volume-based schemes.
Healthpayers should embrace provider behavioral analytics that enable real-time detection of outlier ordering patterns that may be indicative of fraud. It’s likely that DME providers are getting away with obvious methods of fraud, such as ordering hundreds of identical devices. This not-so-subtle behavior should not be able to go unchecked in real-time when it can be stopped prior to claims payment.
DME fraud, like some other healthcare fraud, is more easily illuminated by having cross-payer visibility. Fraud patterns do not hide as easily when data is shared across Medicare, Medicaid, and commercial healthpayers.
Fighting DME Fraud Zombies
DME fraud persists because it still pays. Claims are paid faster than they can be validated, and fraud schemes scale faster than they can be linked and detected, thus the model still works. Bad actors are eventually caught, and new ones will continue to take their place until we change the system. That is why DME is the zombie that never dies.




